
Slides TCTAP
[April 25] CTO LIVE_Asan Medical Center, Seoul, Korea: Case #2
- Operator : Yasushi Asakura
1st Operator: Yasushi Asakura / 2nd Operator: Yong-Rak Cho
Brief Case Summary
A 49 year-old male was admitted for the evaluation of Coronary CT angiography abnormality. The coronary angiography was performed, which reveled significant stenosis LM to proximal LAD, and CTO lesion proximal RCA. Then, LM to proximal LAD lesion was stented.
Past Medical History
- Previous MI: N
- Previous CABG : N
- Previous PCI: Y
- Other: Hyperlipidemia, Current smoker
Demographic Characteristics
- Diabetes: N
- Hypertension: N
- Hyperlipidemia: Y
- Smoking: Y
- Family History: N
- Age: 49
- Sex: Male
Clinical Presentation
Silent ischemia
Non-invasive Studies
Echocardiography
No RWMA with normal LV systolic function (EF 62%)
Treadmill test
Not done
Thallium SPECT
Normal
Cardiac Catheterization Findings
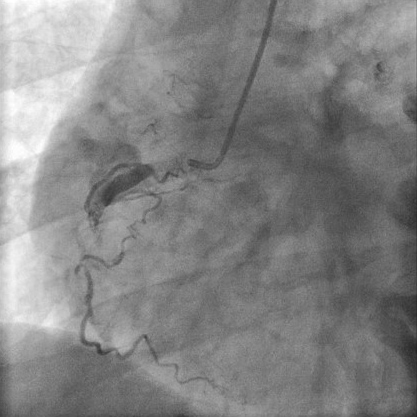
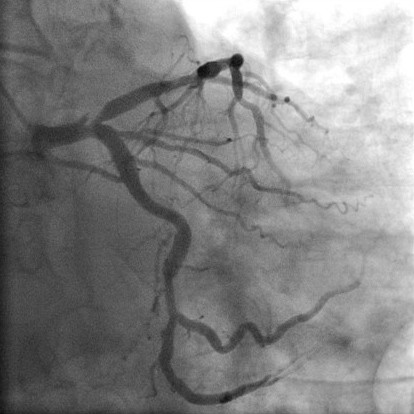
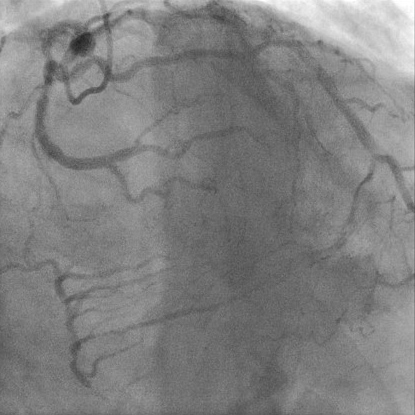
- The coronary angiography showed total occlusion at proximal RCA with grade 3 collateral flow from distal LAD.
- Significant stenosis of LM to proximal LAD was also shown.
- SYNTAX score: 29
Case Notes
Target Lesion(s)
Proximal RCA
Adjunctive Medication
- ASA: Y
- LMWH: N
- Clopidogrel: Y
- Heparin: N
- Nitrates: N
- IIb/IIIa: N
- Other: Beta-blocker, Calcium channel blocker, statin
Teaching Points
- Anterograde or retrograde approach of total occlusion of RCA
Coronary Angiography

- Previous MI: N
- Previous CABG : N
- Previous PCI: Y
- Other: Hyperlipidemia, Current smoker
- Diabetes: N
- Hypertension: N
- Hyperlipidemia: Y
- Smoking: Y
- Family History: N
- Age: 49
- Sex: Male
Echocardiography
No RWMA with normal LV systolic function (EF 62%)Treadmill test
Not doneThallium SPECT
Normal- The coronary angiography showed total occlusion at proximal RCA with grade 3 collateral flow from distal LAD.
- Significant stenosis of LM to proximal LAD was also shown.
- SYNTAX score: 29
Target Lesion(s)
Proximal RCA- ASA: Y
- LMWH: N
- Clopidogrel: Y
- Heparin: N
- Nitrates: N
- IIb/IIIa: N
- Other: Beta-blocker, Calcium channel blocker, statin
- Anterograde or retrograde approach of total occlusion of RCA
Leave a comment