

News | TCTAP 2022
Similarities, differences between EBC MAIN and DKCRUSH-V
Shaoliang Chen, MD compares two major PCI trials on provisional stenting and DK Crush to treat LM bifurcations at TCTAP 2022
Optimal treatment of left main (LM) bifurcation lesions during percutaneous coronary intervention (PCI) may depend on anatomy, evidenced by analysis of the EBC MAIN and DKCRUSH-V trials on provisional- and two-stenting.
Optimal treatment of LM bifurcations remains controversial. Although provisional stenting is the conventional method of treatment, recent studies from Chinese investigators demonstrated that two-stenting with the Double Kissing (DK) Crush technique outperformed provisional stenting.
The 2018 European Society of Cardiology and European Association for Cardio-Thoracic Surgery (ESC/EACTS) guideline on myocardial revascularization has since recommended DK Crush over provisional T-stenting for true LM bifurcation lesions (Class IIb, B).
The 2011 American College of Cardiology Foundation, American Heart Association and Society for Cardiovascular Angiography and Interventions (ACCF/AHA/SCAI) guideline also recommends two-stenting for complex bifurcations (Class IIa, B) but recommends provisional stenting as the initial approach for bifurcation lesions when the side branch (SB) is not large and for mild to moderate focal ostial disease (Class I, A).
Although differences in data and perspectives fueled a divide, analyses of trials on the respective stenting techniques have created a more holistic perspective on the optimal treatment for LM bifurcations that incorporate coronary anatomy.
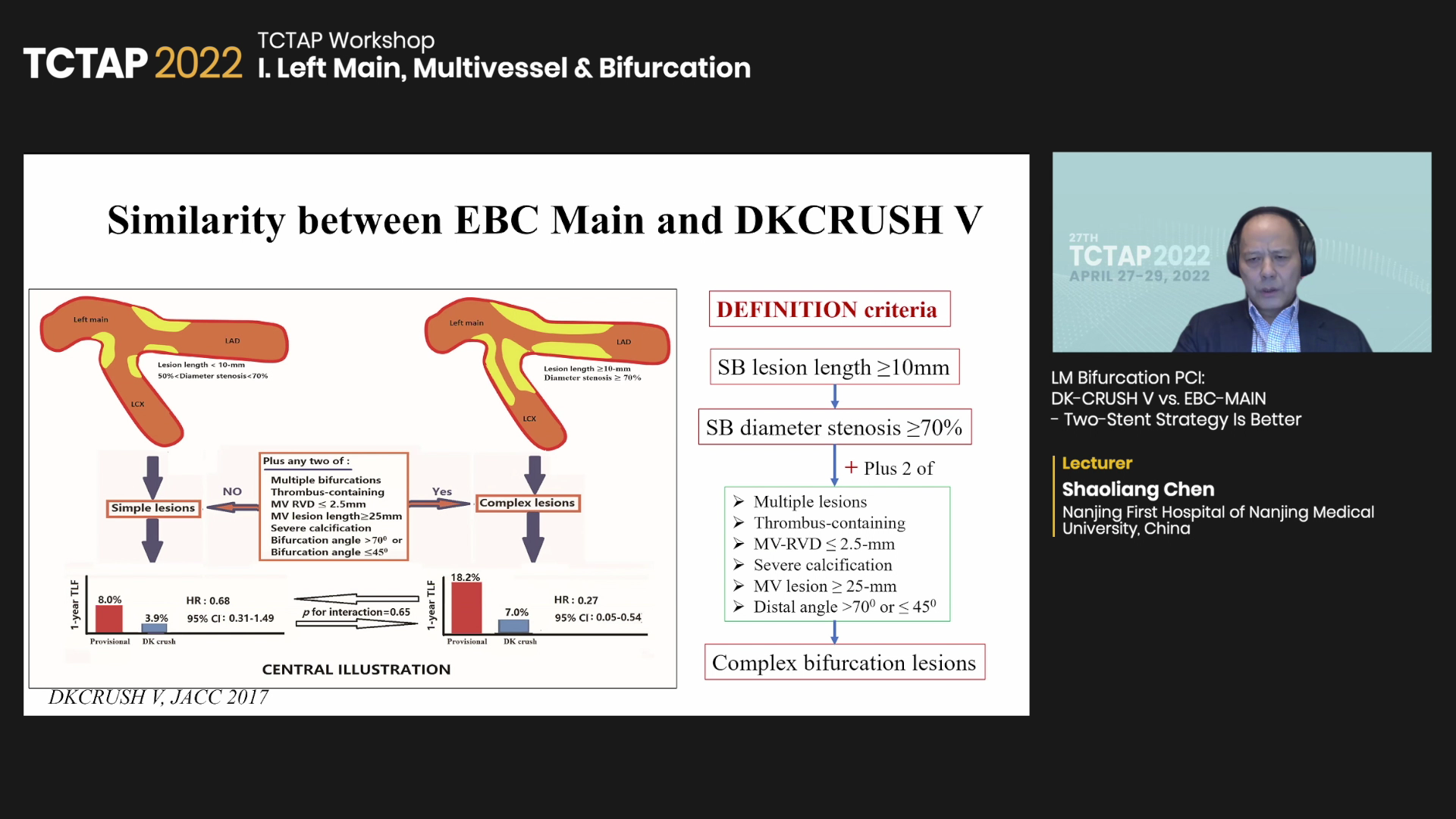
 “Both investigators and cardiologists agree that provisional stenting is better for simple distal LM lesions defined by DEFINITION criteria,” Shaoliang Chen, MD, PhD(Nanjing Medical University, Jiangsu, China) said at TCTAP 2022 on Apr 27.
“Both investigators and cardiologists agree that provisional stenting is better for simple distal LM lesions defined by DEFINITION criteria,” Shaoliang Chen, MD, PhD(Nanjing Medical University, Jiangsu, China) said at TCTAP 2022 on Apr 27.
“But I suggest the two-stent technique, particularly DK Crush, for complex LM lesions when SB lesion length is greater or equal to 10 mm, SB diameter stenosis is greater or equal to 70%, and two other high-risk factors are present” he said.
Comparison of the two trials showed that both were designed to test for superiority and had a similar sample size (EBC MAIN: 467 vs. DKCRUSH-V: 482).
But the studies diverged in the use of two-stent techniques. In EBC MAIN, culotte was used most frequently in the two-stent arm (53%), followed by the T and protrusion (TAP) (33%) and DK Crush (5%). On the other hand, DKCRUSH-V used only the DK Crush technique (100%).
The 1-year primary endpoint event criteria also differed with EBC Main defining composite outcomes as all-cause death, myocardial infarction (MI) and target-lesion revascularization (TLR), and DKCRUSH-V inclduing cardiac death, target-vessel MI (TVMI) and TLR.
EBC MAIN also assumed a “very high” 1-year primary endpoint rate of 25% in the two-stent arm compared to the 7% assumed rate of DKCRUSH-V. Other differences included SYNTAX scores (EBC MAIN: <32 vs. DKCRUSH-V: no limit) and rates of acute MI and chronic total occlusion (CTO).
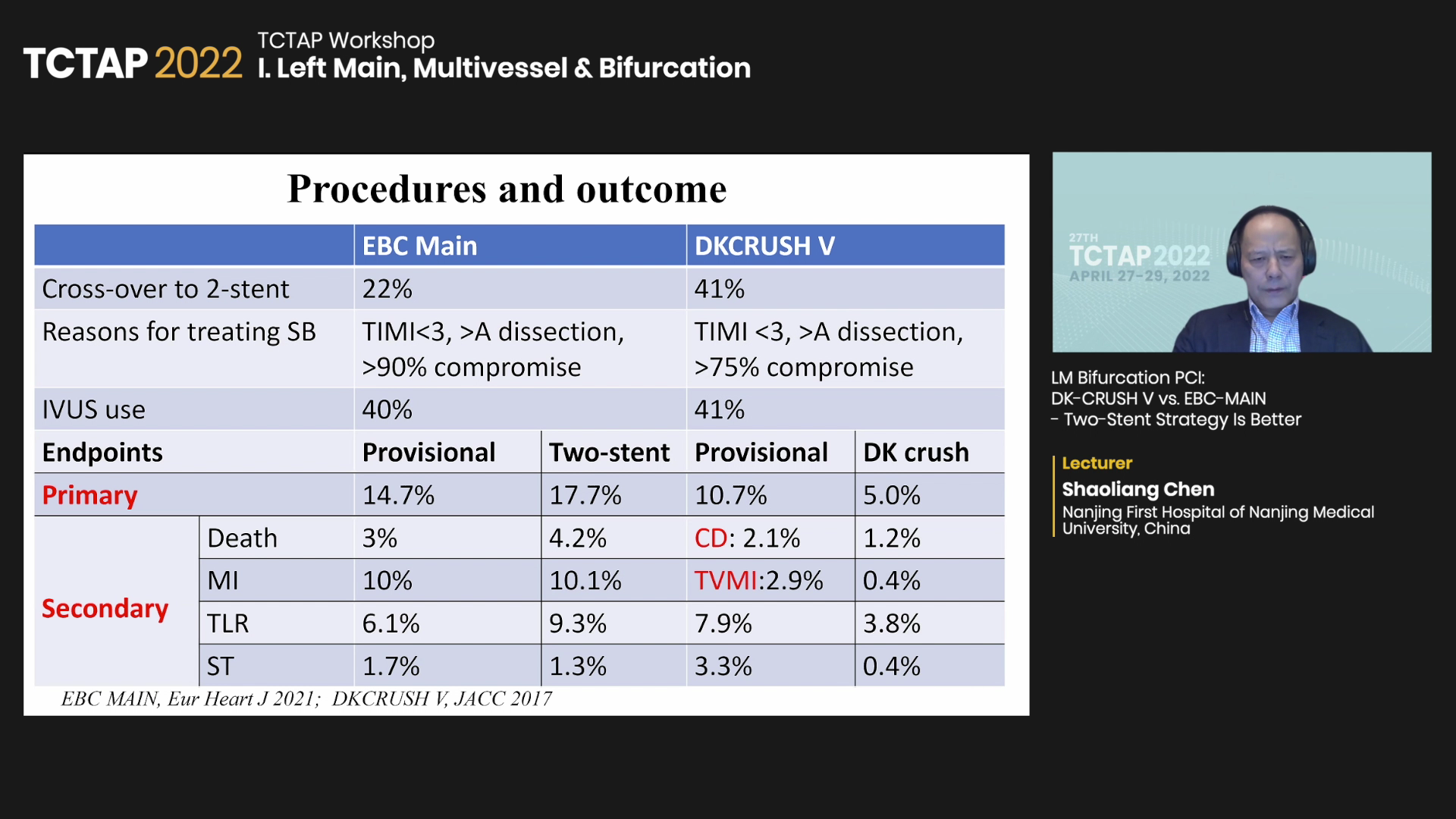
At 1-year follow-up, cross-over to the two-stent arm in EBC MAIN was about half of DKCRUSH-V’s (22% vs. 41%). Both had similar reasons for treating the side branch (>A dissection, TIMI <3, >75~90% compromise). Intravascular ultrasound (IVUS) use was about 40% in both studies.
Chen noted that absolute TLR rates (EBC MAIN: 6.1% vs. DKCRUSH-V: 7.9%) were “a bit high” in DKCRUSH-V but emphasized that 32% of lesions in DKCRUSH-V were complex bifurcations, indicating the 1-year TLR rates were similar between trials.
Edited by

Kyusup Lee, MD
The Catholic University of Korea, Daejeon St. Mary's Hospital, Korea (Republic of)
Written by

YoonJee Marian Chu, Medical Journalist
Read Biography
Chen, Shao-Liang, et al. “Double Kissing Crush versus Provisional Stenting for Left Main Distal Bifurcation Lesions.” Journal of the American College of Cardiology,.
Hildick-Smith, David, et al. “The European Bifurcation Club Left Main Coronary Stent Study: A Randomized Comparison of Stepwise Provisional VS. Systematic Dual Stenting Strategies (EBC Main).” European Heart Journal,.
Optimal treatment of left main (LM) bifurcation lesions during percutaneous coronary intervention (PCI) may depend on anatomy, evidenced by analysis of the EBC MAIN and DKCRUSH-V trials on provisional- and two-stenting.
Optimal treatment of LM bifurcations remains controversial. Although provisional stenting is the conventional method of treatment, recent studies from Chinese investigators demonstrated that two-stenting with the Double Kissing (DK) Crush technique outperformed provisional stenting.
The 2018 European Society of Cardiology and European Association for Cardio-Thoracic Surgery (ESC/EACTS) guideline on myocardial revascularization has since recommended DK Crush over provisional T-stenting for true LM bifurcation lesions (Class IIb, B).
The 2011 American College of Cardiology Foundation, American Heart Association and Society for Cardiovascular Angiography and Interventions (ACCF/AHA/SCAI) guideline also recommends two-stenting for complex bifurcations (Class IIa, B) but recommends provisional stenting as the initial approach for bifurcation lesions when the side branch (SB) is not large and for mild to moderate focal ostial disease (Class I, A).
Although differences in data and perspectives fueled a divide, analyses of trials on the respective stenting techniques have created a more holistic perspective on the optimal treatment for LM bifurcations that incorporate coronary anatomy.
“Both investigators and cardiologists agree that provisional stenting is better for simple distal LM lesions defined by DEFINITION criteria,” Shaoliang Chen, MD, PhD(Nanjing Medical University, Jiangsu, China) said at TCTAP 2022 on Apr 27.
“But I suggest the two-stent technique, particularly DK Crush, for complex LM lesions when SB lesion length is greater or equal to 10 mm, SB diameter stenosis is greater or equal to 70%, and two other high-risk factors are present” he said.
Comparison of the two trials showed that both were designed to test for superiority and had a similar sample size (EBC MAIN: 467 vs. DKCRUSH-V: 482).
But the studies diverged in the use of two-stent techniques. In EBC MAIN, culotte was used most frequently in the two-stent arm (53%), followed by the T and protrusion (TAP) (33%) and DK Crush (5%). On the other hand, DKCRUSH-V used only the DK Crush technique (100%).
The 1-year primary endpoint event criteria also differed with EBC Main defining composite outcomes as all-cause death, myocardial infarction (MI) and target-lesion revascularization (TLR), and DKCRUSH-V inclduing cardiac death, target-vessel MI (TVMI) and TLR.
EBC MAIN also assumed a “very high” 1-year primary endpoint rate of 25% in the two-stent arm compared to the 7% assumed rate of DKCRUSH-V. Other differences included SYNTAX scores (EBC MAIN: <32 vs. DKCRUSH-V: no limit) and rates of acute MI and chronic total occlusion (CTO).
At 1-year follow-up, cross-over to the two-stent arm in EBC MAIN was about half of DKCRUSH-V’s (22% vs. 41%). Both had similar reasons for treating the side branch (>A dissection, TIMI <3, >75~90% compromise). Intravascular ultrasound (IVUS) use was about 40% in both studies.
Chen noted that absolute TLR rates (EBC MAIN: 6.1% vs. DKCRUSH-V: 7.9%) were “a bit high” in DKCRUSH-V but emphasized that 32% of lesions in DKCRUSH-V were complex bifurcations, indicating the 1-year TLR rates were similar between trials.
Edited by
Kyusup Lee, MD
The Catholic University of Korea, Daejeon St. Mary's Hospital, Korea (Republic of)
Written by
YoonJee Marian Chu, Medical Journalist
Read BiographyChen, Shao-Liang, et al. “Double Kissing Crush versus Provisional Stenting for Left Main Distal Bifurcation Lesions.” Journal of the American College of Cardiology,.
Hildick-Smith, David, et al. “The European Bifurcation Club Left Main Coronary Stent Study: A Randomized Comparison of Stepwise Provisional VS. Systematic Dual Stenting Strategies (EBC Main).” European Heart Journal,.
Leave a comment