
News | TCTAP 2024
TAVR-in-TAVR: The NEXT Challenging Issue in Lifetime TAVR Management
TAVR: Key Issues in 2024

Philippe Garot
Institut Cardiovasculaire Paris-Sud, France
Compared to surgical aortic valve replacement (SAVR), there is an increasing use of transcatheter aortic valve replacement (TAVR) in patients over 80 years old, as well as in those aged 65-80 years in western countries. In patients with a remaining life-expectancy of over 10 years, a considerable number of transcatheter heart valves (THVs) are expected to fail, requiring repeat intervention. According to a multicenter registry, surgical explantation after TAVR failure was associated with an overall mortality of almost 15% at 30 days and 30% at 1 year follow-up. Contrastingly, redo-TAVR is relatively safe and effective. Underexpansion of THVs may lead to hypoattenuated leaflet thickening (HALT) and early dysfunction with elevated gradients. In these patients, a staged post-dilation of the THVs may improve hemodynamics and delay a redo-TAVR procedure.
Coronary access may be impaired after a redo-TAVR procedure. Factors impacting coronary access may be anatomical, or related to the device and the procedure. The design of the index TAVR implant is associated with a different risk of sinus sequestration and coronary obstruction. The risk of sinus sequestration increases up to 91% in balloon-expandable valve (BEV)-in-self-expandable valve (SEV) and 75% in SEV-in-SEV, and in these cases, leaflet interventions should be considered as a prerequisite for redo-TAVR (Figure 1 ).
The optimal THV design and implantation technique for redo-TAVR are poorly understood. In the case of redo-TAVR, the leaflets of the failed THV may create a “tube graft,” where the index THV leaflets can be jailed between the two THV frames. This can create a neoskirt of tissues from the failed THV inflow to the top of the jailed leaflet, which may limit subsequent coronary access and flow. The higher the second THV, the taller the neoskirt, with a higher risk of sinus sequestration.
The position of both the index and the second THV are crucial in avoiding sinus sequestration. In some patients, the second implant must be lower to avoid a tall neoskirt, causing a significant leaflet overhang in return. The width of the sinuses of Valsalva is a key for a reasonable valve-to-coronary (VTC) distance, which may be compromised by THV flaring, second implant depth and valve canting. The risk of coronary obstruction after redo-TAVR is strongly related to the index TAVR design, the implant depth of the index THV and commissural alignment of both the index and redo-THV, which can help avoiding coronary obstruction and facilitate leaflet interventions. Also, the index failed THV may expand after redo-TAVR, and this should be considered when determining the VTC distance.
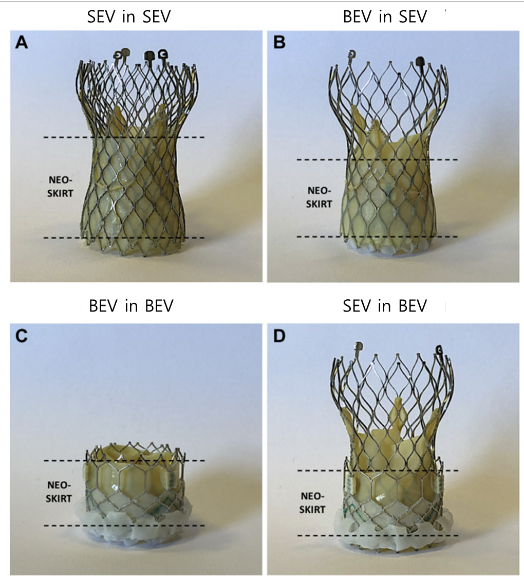
Figure 1. Different THV-in-THV combinations and the neoskirt heights
TCTAP Workshops
TAVR: Key Issues in 2024
Thursday, April 25, 10:30 AM ~ 11:25 AM
Presentation Room 1, Level 1
Edited by

Cheol Hyun Lee, MD
Keimyung University Dongsan Medical Center, Korea (Republic of)
Philippe Garot
Institut Cardiovasculaire Paris-Sud, France
Compared to surgical aortic valve replacement (SAVR), there is an increasing use of transcatheter aortic valve replacement (TAVR) in patients over 80 years old, as well as in those aged 65-80 years in western countries. In patients with a remaining life-expectancy of over 10 years, a considerable number of transcatheter heart valves (THVs) are expected to fail, requiring repeat intervention. According to a multicenter registry, surgical explantation after TAVR failure was associated with an overall mortality of almost 15% at 30 days and 30% at 1 year follow-up. Contrastingly, redo-TAVR is relatively safe and effective. Underexpansion of THVs may lead to hypoattenuated leaflet thickening (HALT) and early dysfunction with elevated gradients. In these patients, a staged post-dilation of the THVs may improve hemodynamics and delay a redo-TAVR procedure.
Coronary access may be impaired after a redo-TAVR procedure. Factors impacting coronary access may be anatomical, or related to the device and the procedure. The design of the index TAVR implant is associated with a different risk of sinus sequestration and coronary obstruction. The risk of sinus sequestration increases up to 91% in balloon-expandable valve (BEV)-in-self-expandable valve (SEV) and 75% in SEV-in-SEV, and in these cases, leaflet interventions should be considered as a prerequisite for redo-TAVR (Figure 1 ).
The optimal THV design and implantation technique for redo-TAVR are poorly understood. In the case of redo-TAVR, the leaflets of the failed THV may create a “tube graft,” where the index THV leaflets can be jailed between the two THV frames. This can create a neoskirt of tissues from the failed THV inflow to the top of the jailed leaflet, which may limit subsequent coronary access and flow. The higher the second THV, the taller the neoskirt, with a higher risk of sinus sequestration.
The position of both the index and the second THV are crucial in avoiding sinus sequestration. In some patients, the second implant must be lower to avoid a tall neoskirt, causing a significant leaflet overhang in return. The width of the sinuses of Valsalva is a key for a reasonable valve-to-coronary (VTC) distance, which may be compromised by THV flaring, second implant depth and valve canting. The risk of coronary obstruction after redo-TAVR is strongly related to the index TAVR design, the implant depth of the index THV and commissural alignment of both the index and redo-THV, which can help avoiding coronary obstruction and facilitate leaflet interventions. Also, the index failed THV may expand after redo-TAVR, and this should be considered when determining the VTC distance.
TCTAP Workshops
TAVR: Key Issues in 2024
Thursday, April 25, 10:30 AM ~ 11:25 AM
Presentation Room 1, Level 1
Edited by
Cheol Hyun Lee, MD
Keimyung University Dongsan Medical Center, Korea (Republic of)
Leave a comment